Clients rely on skin health professionals to answer their questions accurately and honestly. Clinical estheticians are often faced with treating more than hyperpigmentation, acne, rosacea and visible aging because additional dermatological irregularities and curiosities are commonly brought to their attention. Although many cutaneous concerns should be treated by a physician, being able to identify various lesions can be helpful to the esthetician in developing treatment plans and determining when to refer to a physician for suspicious abnormalities. There is often a fine line between conditions that are dangerous and those that are merely cosmetically bothersome—understanding the difference is crucial to healthy, happy clients.
As the protective barrier for the body, the skin is constantly exposed to various offenders. The amount of stress placed on this vital organ often results in various physiological changes. The pathway in which these conditions are formed—and whether or not they spread and damage surrounding tissue—determines the level of threat they are to the overall health of the client. Noncancerous skin growths, such as seborrheic keratoses, sebaceous hyperplasias, cherry hemangiomas and verrucae planae (flat warts) are examples of skin concerns that are visually unappealing but not considered harmful. Cancerous lesions such as basal cell carcinomas, squamous cell carcinomas and melanomas, as well as those lesions with the potential of progressing into skin cancer, such as actinic keratoses, can be life-threatening in some circumstances.
Cause for concern
Skin cancer is the most common type of cancer in the United States, and its various presentations can make it difficult to identify without proper physician examination. Cancerous lesions invade and destroy surrounding normal skin cells and tissues and, although prevention by using daily sunscreen and antioxidants is best, appropriate treatment is crucial once any type of skin cancer develops. Any and all questionable skin growths should be examined by a dermatologist before topical treatment is applied.
Actinic keratoses (AK). These are abnormal growths resulting from overexposure to UV rays. AK are considered pre-cancerous and, if left untreated, they can develop into squamous cell carcinomas (SCC). The appearance of AKs is rough and scaly, and they can be tan, red, pink or flesh-colored. Studies show that up to 60% of SCC begins as AK.1 They can be treated by physicians in several ways, including cryosurgery (freezing of the lesions), curettage (scraping of abnormal surface tissue), 5-aminolevulenic acid photodynamic therapy (PDT), surgical excision and topical destructive cream medications. Clinical studies have also shown chemical peels, such as Jessner’s solutions and trichloroacetic acids (TCA) preparations, to be effective treatments as well.2
Basal cell carcinoma (BCC). They can be as simple as a tiny, clear, pearly or flesh-colored bump or may be more apparent, such as an open sore or shiny red, pink, brown or black lesion that can be mistaken for a mole. Although BCC is considered the least threatening form of skin cancer because it grows the slowest and is the least likely to metastasize, or spread, it can be incredibly locally destructive or disfiguring.
Squamous cell carcinoma (SCC). This has a red, rough or flaky appearance and often causes thickening of the skin. Ulcerations may occur and cause a chronic open sore. SCC primarily affects the superficial layers of the epidermis and approximately 97% of SCC does not spread; however, if metastasis does occur, scarring, disfigurement or death is possible.3
Melanoma. This is a dark-colored cancer of the skin’s pigment-producing cells, known as melanocytes. This is the most dangerous form of skin cancer due to its ability to metastasize and spread to lymph nodes, blood, distant tissues and organ systems. If detected and treated early while it is still thin, melanoma can typically be cured. Once it spreads, melanoma can be extremely difficult to treat and often leads to death. If a mole presents any of these characteristics, or if it changes in size, shape, color or texture, it should be emphasized to the client to have it evaluated by a dermatologist in the near future.
Cosmetic annoyances
The following skin concerns are completely benign. Although they will not cause harm, many require special treatment considerations. Many of these harmless lesions look similar to skin cancers; therefore, it is important that nonphysician skin care professionals have their clients properly diagnosed by a knowledgeable physician.
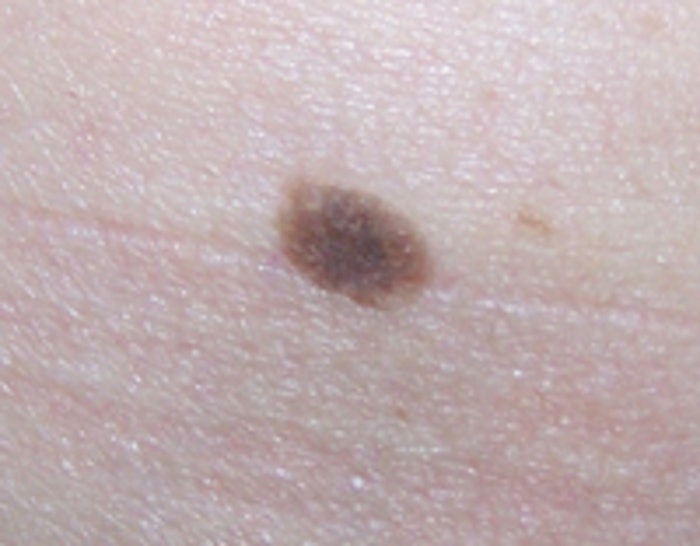
Moles. These are a completely normal part of human anatomy, and most adults will have 10–40 moles.4 Although they can be flesh-colored, the majority are dark in color because of the involvement of pigmented melanocytes in their development. Moles occur when multiple melanocytes grow bunched together. Although many moles are normal and harmless, clients prone to the development of moles are also more prone to skin cancer. Any mole that changes in size, color or shape should be examined to ensure it is not cancerous. If removal is desired—even if just for cosmetic reasons—moles should be surgically excised and examined by a pathologist.
Seborrheic keratoses (SK). These are typically dark-colored lesions that appear to be stuck on the surface of the skin. They are waxlike and often have a rough, uneven texture. SK are considered to be the most common noncancerous dermatological concern. They can be found anywhere on the body, but are more commonly found in sun-exposed areas. SK are not contagious and although their exact cause is unknown, they seem to be linked to heredity. Studies show that, although patients with SK can develop skin cancer and SK can look strikingly similar to skin cancer, this type of keratosis does not progress into a cancerous lesion.5 SK should be removed by a physician using electrocautery (burning the lesion with electric currents), cryosurgery or curettage. Treatment with chemical peels or microdermabrasion will not cause harm; however, complete clearance of SK is not typically possible with these methods of treatment.
Sebaceous hyperplasias. These result from an abnormal enlargement of the sebaceous gland and are thought to affect nearly 1% of the U.S. population.6 These yellow or orange lesions are most common on the forehead, nose and cheeks because of the abundance of oil glands in these areas of the face. Sebaceous hyperplasias can be mistaken for BCC due to their raised, nodular, bumpy appearance. The term hyperplasia describes the abnormal buildup of cells. They are believed to be caused by the decrease in cell turnover associated with the aging process. Sebocytes, or cells that form the sebaceous glands, mature and then eventually dissolve, releasing oily sebum. Sebaceous hyperplasias form when these sebocytes do not break down and, instead, crowd the oil gland, causing it to expand. Research indicates that sebaceous hyperplasias are not linked to skin carcinogenesis in any way.7 There are several treatment methods available, including cryotherapy, electrocautery, curettage, laser treatments, phytodynamic therapy, and topical treatment using TCA acid and retinoids. Sebaceous hyperplasia may reoccur if not completely removed.
Cherry hemangiomas. These are caused by an abnormal gathering of dilated small blood vessels called venules. This type of lesion is typically small and round and ranges in color from bright red to purple. They can be smooth or raised to the touch. The probability of developing cherry hemangiomas increases with age, and they can appear anywhere on the face or body. There is no link between cherry hemangiomas and skin cancer; however, some more vascular BCC and SCC can have a similar appearance to this common vascular lesion so a physician should always be consulted for proper diagnosis. Cautery and light therapy treatment are the best options. With these types of treatments an electrical hyfrecator, or laser or intense pulsed light (IPL) beam cauterizes the vascular lesion, causing it to disintegrate.
Verrucae planae. These are flat warts. All types of warts are caused by the human papillomavirus and, unlike common warts, flat warts often appear on the face. This particular type of wart tends to be less obvious than other warts but can proliferate in large numbers. Although warts are completely benign and not linked to skin cancer, they are contagious. Compromised skin is more susceptible to contracting the virus and cross-contamination is a risk; therefore, full-face treatments should not be performed on clients with verrucae planae present on the skin. Flat warts can be broken down by acidic preparations, including salicylic, glycolic and retinoic acids and these types of ingredients are often used as a spot treatment. Additional treatment options include: cryotherapy, laser, a chemical called cantharidin and the topical medication imiquimod.
It’s not just esthetics
Trust is the most important aspect of the client-esthetician relationship. Being able to offer more insight into all skin concerns—not just the esthetic—instantly boosts credibility and deepens this trust. Being honest and knowing when treatment is out of your realm of expertise will encourage clients to trust your recommendations. Moreover, estheticians have the ability to save lives. By carefully evaluating each client’s skin and referring to a dermatologist whenever anything appears abnormal, estheticians can help in the early diagnosis of dangerous cancerous lesions.
REFERENCES
1. A Berner, Actinic keratosis and development of cutaneous squamous cell carcinoma, Tidsskr Nor Laegeforen 125 12 1653–1654 (2005)
2. N Lawrence, SE Cox, C Cockerell, et al, A comparison of the efficacy and safety of Jessner’s solution and 35% trichloroacetic acid vs 5% fluorouracil in the treatment of widespread facial actinic keratoses, Arch Dermatol 131 176–181 (1995)
3. www.skincancer.org/scc-treatment-options.html
4. www.cancer.gov/cancertopics/wyntk/moles-and-dysplastic-nevi/allpages
5. B Lindelof, B Sigurgeirsson and S Melander, Seborrheic keratoses and cancer, J Am Acad Dermatol 1992 26 6 947–950 (1992)
6.emedicine.medscape.com/article/1059368-overview
7. DJ Day, 100 Questions & Answers about Acne, Jones and Bartlett, Sudbury, MA (2005)
(All websites accessed Dec 8, 2010)
After completing her fellowship in Mohs micrographic surgery, dermatologic, laser and cosmetic surgery in 2004, Jennifer Linder, MD, joined the Laser & Cosmetic Surgery Institute in Greenbrae, California, where she performed and oversaw thousands of laser and aesthetic procedures. In 2006 she began her own practice in Scottsdale, Arizona, which has now grown to be one of the busiest dermatology and Mohs surgery centers in Arizona. In addition, Linder is the chief scientific officer for PCA Skin, overseeing all research and development and clinical trial processes.
Cause for concern 1
Squamous cell carcinoma

Cause for concern 2
Basal cell carcinoma

Cosmetic annoyances 1
Moles

Cosmetic annoyances 2
Seborrheic keratoses

Cosmetic annoyances 3
Sebaceous hyperplasias

Cosmetic annoyances 4
Cherry hemangiomas

Cosmetic annoyances 5
Verrucae planae